
Redesigning the NHS Electronic Referral Service (e-RS)
I am the Design Lead for a project to improve the end-to-end user experience of the NHS’s Electronic Referral Service (e-RS), a critical internal clinical system. This work forms part of a wider NHS initiative to modernise internal services and align them with the NHS Service Standard—making e-RS the first internal service of this scale to do so.
Challenge
e-RS is a digital platform that provides an easy way for referrers and service providers to manage their patients’ journeys. Users can:
- create referrals for patients
- book appointments or select services for triage
- change or cancel appointments
- have advice conversations with other users
- add to and select from the Directory of Services (DOS)
- download and create reports and extracts
Clinical systems are often criticised for poor usability and performance, and the legacy e-RS service is no exception. It is difficult to navigate, requires significant insider knowledge to use effectively, and has long frustrated its 20,000+ daily users. These issues stem largely from the historic lack of evidence-based design, with key design decisions previously driven by senior stakeholders and developers rather than user needs.
What we did
My team and I balance policy intent with user needs in an NHS setting where clinical input is essential to minimising risks to patient care, and where usability itself is a matter of clinical safety.
Throughout this process, the following factors have been instrumental in delivering a significant proportion of the project successfully:
Feature audit
Working with NHS SMEs and our research team, we found that many features were used by only a very small number of users.
This reflected a lack of design thinking in feature prioritisation, resulting in functionality misaligned with most users’ needs. The outcome was a cluttered, sometimes confusing interface that increased cognitive load, especially for new users.
To address this, we analysed feature usage to identify both the most and least frequently used elements.
While decisions about removal were beyond this project’s remit—given e-RS’s role in patient safety—we worked with clinical risk experts to ensure any proposed removals would not endanger patients.
This process refined the scope of necessary changes and enabled the delivery team to plan with greater accuracy and confidence.
Exploring design options
As noted earlier, ensuring this service met the NHS Service Standard was essential. This required us to use predefined styles and components from the NHS Service Manual. While these met most UI needs, the complexity of e-RS exposed certain limitations.
To address these gaps, we looked beyond the NHS Service Manual to the wider gov.uk design system. For example, when we needed a data table with sorting and filtering capabilities, we drew on a solution developed by the Ministry of Justice. Similarly, we made extensive use of HMRC’s timeline component.
Repurposing components in this way brought two key benefits: confidence that they had been thoroughly tested with users and assurance that accessibility requirements were already embedded. More broadly, we believe this approach reflects the open-source, collaborative ethos at the heart of public service design.
Testing the quick wins with the NHS Protoyping Kit
The NHS Prototyping Kit is well-suited for creating prototypes to gather usability metrics for key journeys, particularly those beyond the scope of more complex features.
Using the kit, we prototyped, validated, and iterated core elements such as user login, patient location, and form-based features. In cases where we diverged from NHS Service Manual patterns—acknowledging that not everything we design is a website—we documented both the reasoning and the approach taken.
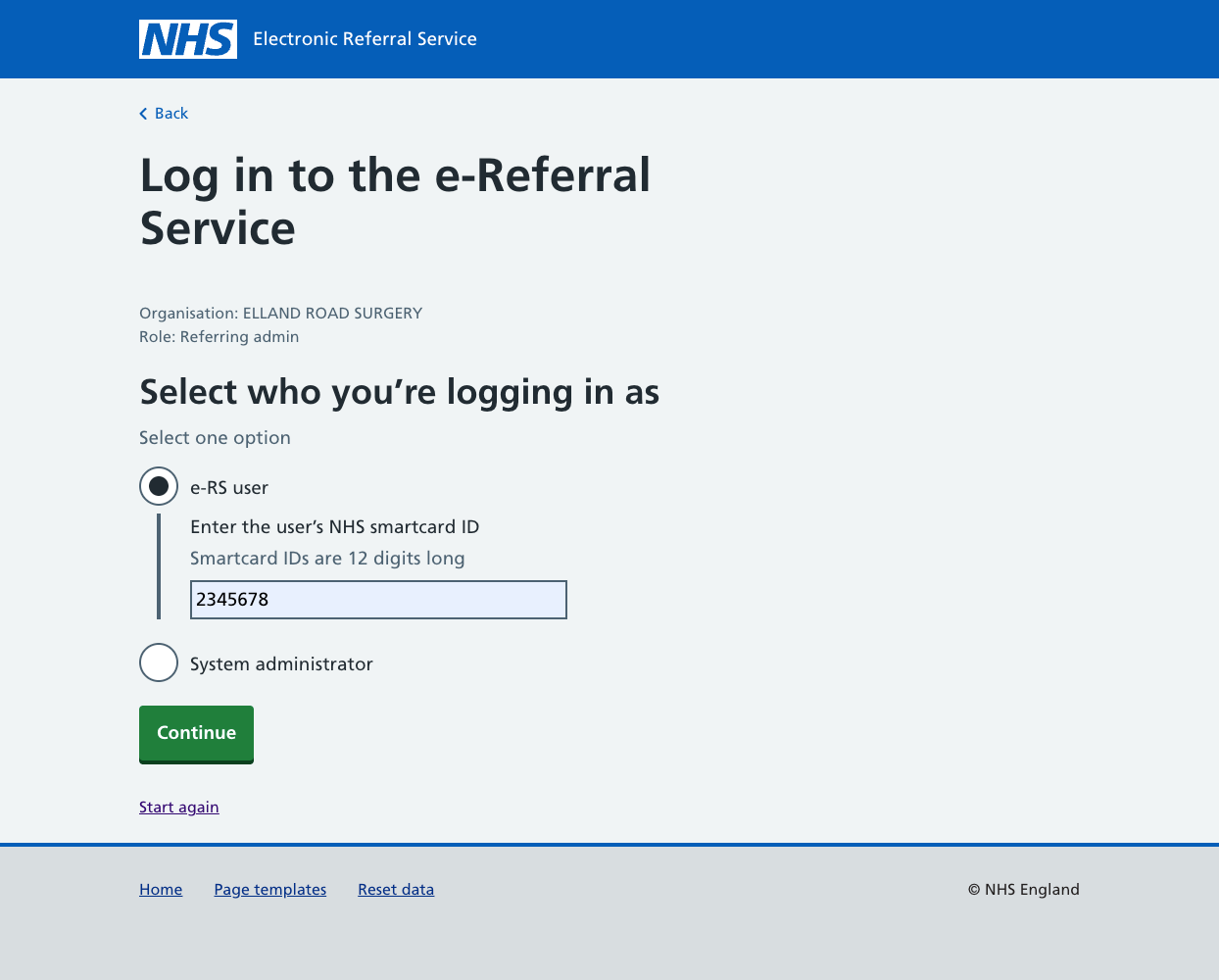
Part of the login journey using the NHS Protyping kit.
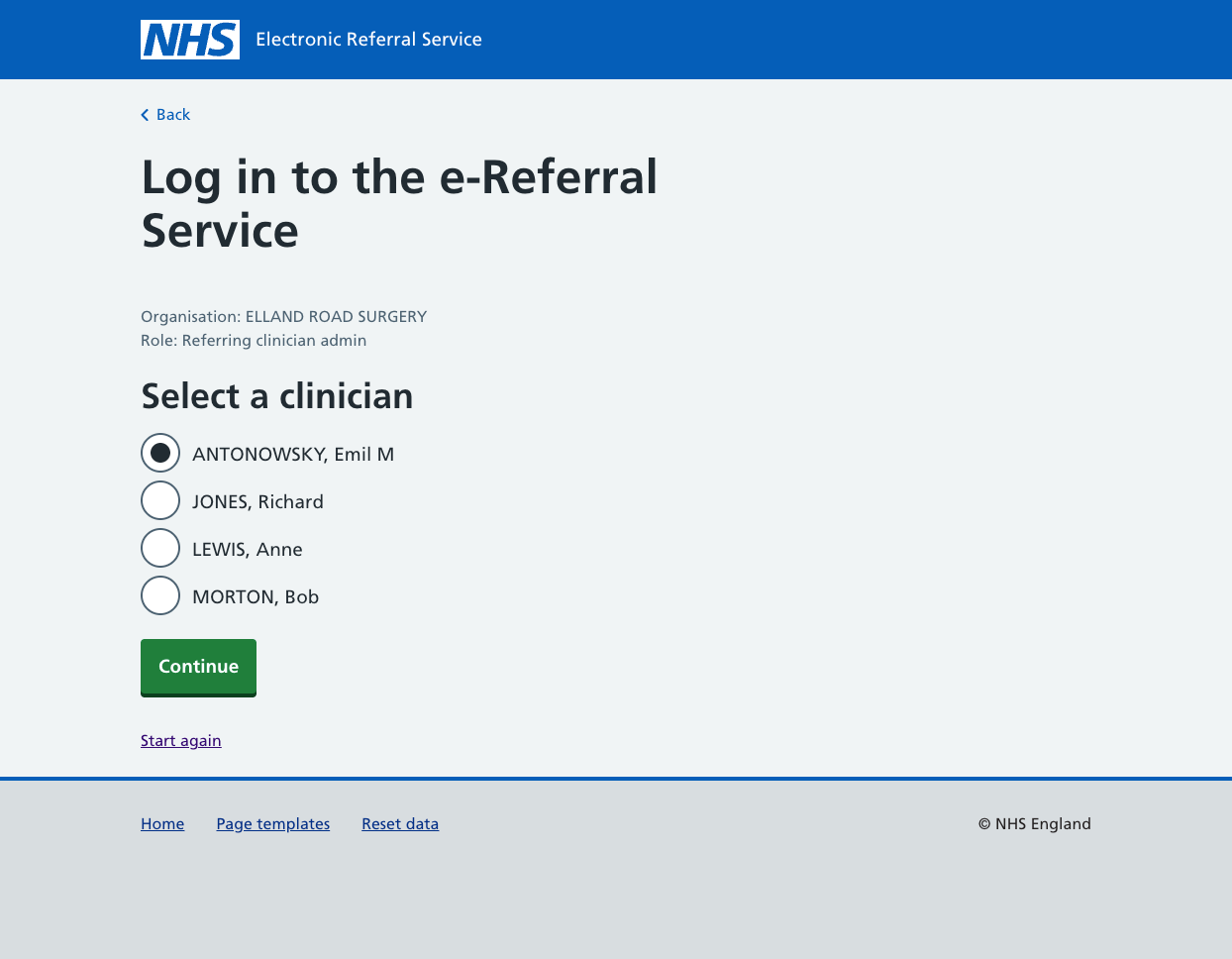
Using routing logic to determine subsequent user journeys.
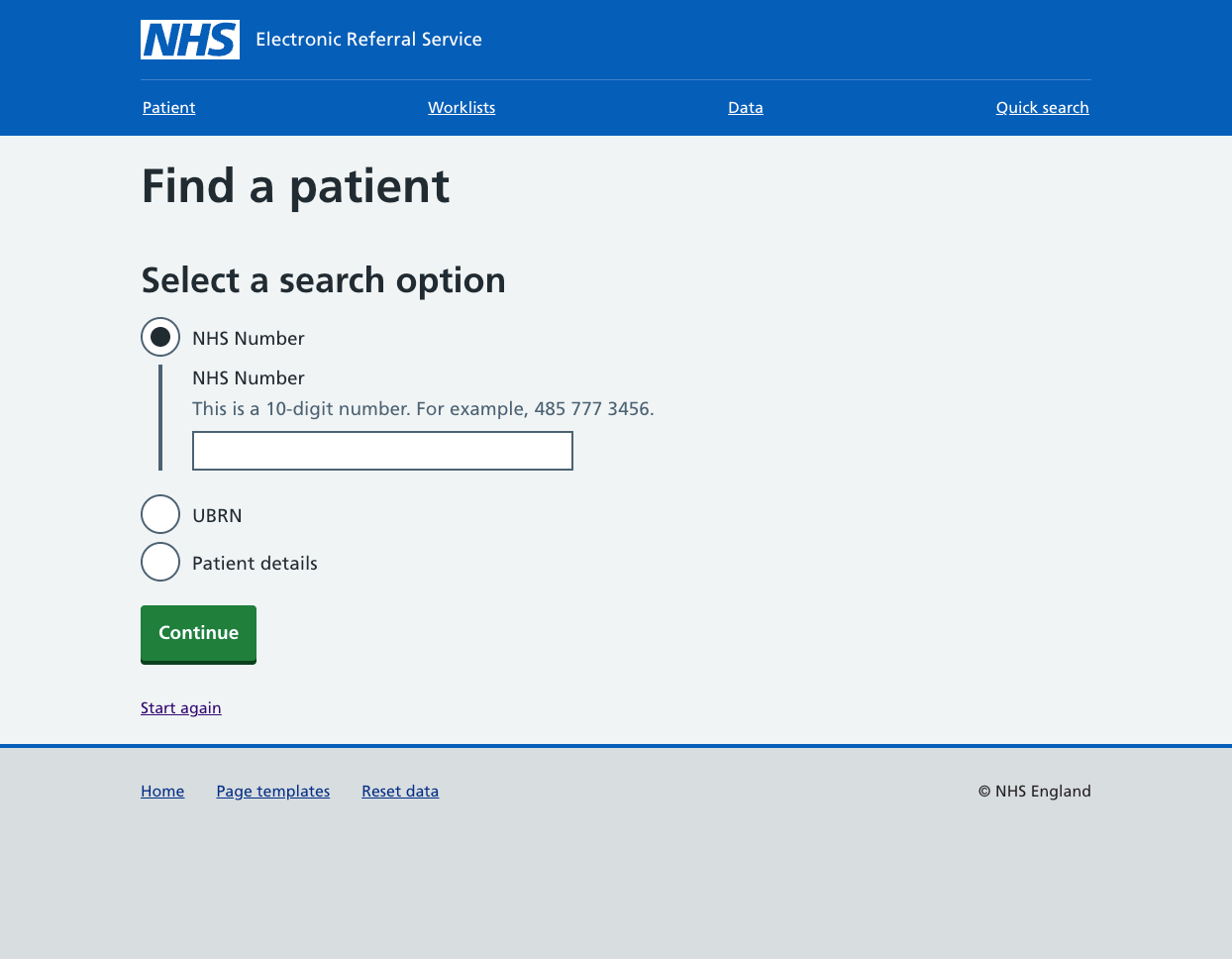
Finding a patient in e-RS using the NHS Prototyping kit.
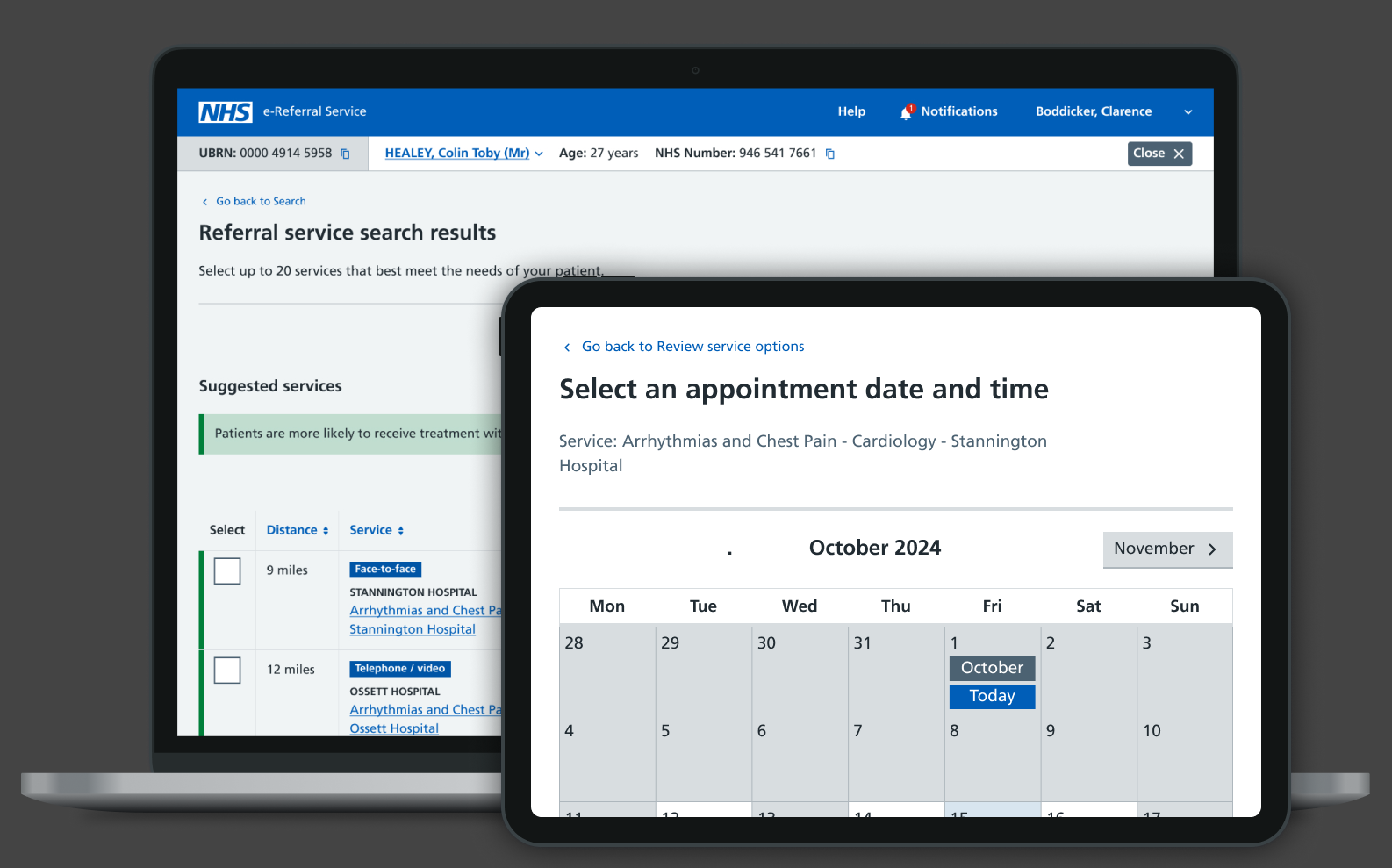
Tackling more complex UI requirements
We hypothesised that the presentation of tabulated data would be critical to the project’s success. A frequent complaint about the legacy service was the poor legibility of tables, often due to small font sizes and users overlooking off-screen data.
Building on the MoJ table component, we developed a fully functional coded prototype and tested it with users. The solution addressed key shortcomings of the original design by introducing sticky headers and columns, improving scrollability, clearly signalling when data extended off-screen, and removing redundant columns. These improvements significantly reduced the risk of important information being missed and formed the basis for subsequent design decisions.
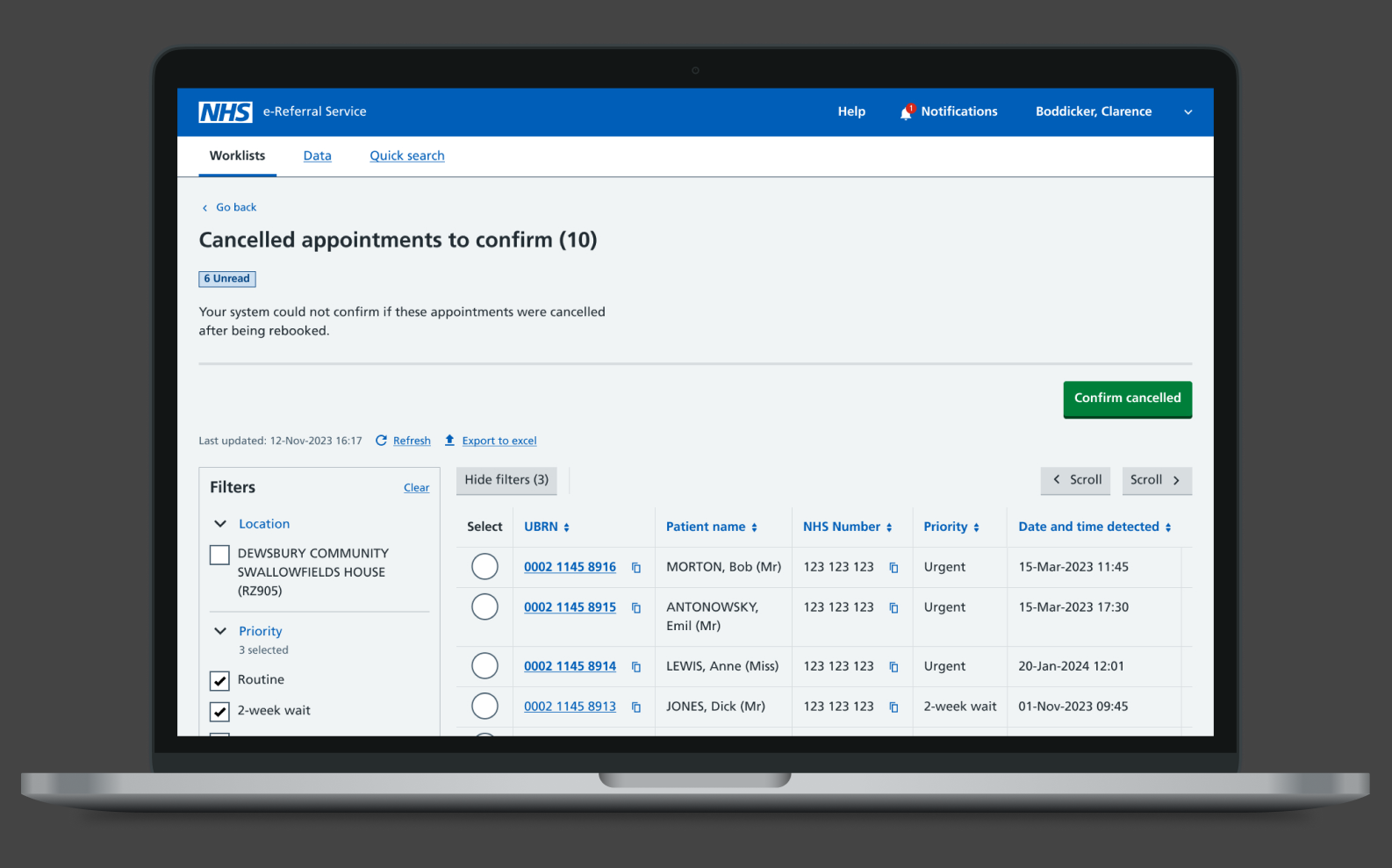
From this foundation, we went on to design more complex tables with filters and column selection, further enhancing usability and flexibility.
The subsequent design decisions were informed by this foundational approach, leading to the creation of complex tables incorporating filters and column selection.

Complex tables with filters and column selection.

Combining a form and table pattern to allow users to make informed selections from a large data-set.

Documenting design components that are specific to e-RS.
My role
In my capacity as a consultant at BJSS, I collaborated with both permanent NHS team members and civil servants. My role was that of Lead Designer. The responsibilities entailed:
Outcomes
TThe project is being delivered to an ambitious schedule, with a streamlined team of interaction designers, a content designer, researchers, developers, and a single Subject Matter Expert proving highly effective. Collaboration has been central, with Figma enabling openness, scrutiny, and smooth sign-off with minimal friction or context-setting.
Now nine months in, the project has received overwhelmingly positive feedback from both the client and users. The next phase will focus on sharing design ideas with the wider NHS design and research community.